If the CMS 2027 Advance Notice has you looking for a prospective risk adjustment solution, we can help. Cozeva and our new partner, Vatica, offer proven methods of risk adjustment that comply with proposed policy changes. We can help you navigate this new landscape and realize prospective risk value in as little as 30 days. We're ready to help. Fill out the form below.
We follow GDPR Privacy Guidelines
We use cookies to enhance your browsing experience. By clicking “Accept and Continue”, you consent to our use of cookies.
Realign your Stars strategy with the right resources
By Rebecca Darnall, MBA, VP of solution development
And Sharalee Johnson, MBA, BSN, RN, CPHQ, VP of customer programs and partnerships
Much of the focus from the 2027 CMS Final Rule has been on rates and risk adjustment. But changes to the Stars program will impact health plans significantly.
Similar to the risk adjustment changes that require primary care practitioner (PCP) involvement and meaningful clinical improvements, the Stars program is moving from administrative optimization to clinical outcomes. Realigning your strategy now will ensure you are ready for future changes.
Focus on clinical outcomes
The rule eliminates 11 administrative measures viewed as “check-the-box” scoring opportunities. To better reflect the actual quality of care delivered, outcomes-based clinical measures will take their place.
Most of these measure removals will apply beginning with the 2029 Star ratings, based on the 2027 measurement year. CMS also finalized earlier removal of Call Center — Foreign Language Interpreter and TTY Availability and Statin Therapy for Patients with Cardiovascular Disease, beginning with the 2028 Star ratings.
A good example is the elevation of depression screening and follow-up as a priority measure, integrating behavioral health into the overall view of the member’s care.
CMS also considered removing additional traditional process measures, including Diabetes Care Eye Exam, but did not finalize that proposal after public comment. This reinforces that the agency is taking a targeted approach, rather than broadly eliminating all preventive care measures.
At the same time, plans should expect continued movement in cut points and measure-level scoring dynamics. With fewer “buffer” measures available, organizations will have less ability to offset underperformance. Success will depend on consistently delivering high-quality outcomes across populations. This means not just closing gaps, but outperforming competitors in a statistically tighter environment.
Patient experience and outcomes will drive performance
CMS is significantly increasing the impact of patient experience (Consumer Assessment of Health Plans Survey) and health outcomes (Health Outcomes Survey) on Star ratings. These measures are expected to account for a substantial portion of overall scoring in the coming years.
Unlike traditional gap closure measures, patient experience and health outcomes measures cannot be addressed through retrospective outreach alone. They reflect the member’s longitudinal experience with the healthcare system, including access, care coordination, communication and functional health outcomes.
This introduces greater variability and elevates the importance of consistent, high-quality interactions at the point of care. Performance will depend on the ability to deliver a reliable, patient-centered experience across the care continuum.
The primary care visit takes center stage
With the focus on clinical outcomes, PCPs are crucial to Stars performance. The primary care encounter, particularly the annual wellness visit and routine follow-ups, is the central point where risk adjustment, quality measurement and outcomes performance converge. This is where plans can have the most impact when partnering with providers to improve risk adjustment accuracy and care gap closure. But it requires plans to enable providers to act on multiple priorities within a single visit via the following:
EHR-integrated workflows: Stars gap prompts and quality alerts must be embedded directly into clinical workflows, not managed through retrospective outreach alone.
Real-time gap visibility and availability: Providers need real-time access to accurate member profiles, including quality, chronic conditions for risk adjustment, and care gap data at the point of care to enable dual-purpose gap closure within a single encounter.
Behavioral health workflows: As noted above, CMS is elevating behavioral health as a core component of overall quality performance, not a standalone measure. Depression screening and follow-up now require structured, repeatable workflows that include screening, documentation, follow-up care and outcome tracking. This positions PCPs as the front line of behavioral health integration, increasing both clinical responsibility and operational complexity.
Stars performance drives overall plan performance and competitiveness
Stars performance is not just a quality metric to support a patient’s wellness; it is a primary financial lever for Medicare Advantage plans, directly impacting revenue, benefit design and long-term growth.
Star ratings influence benchmark payments, rebate percentages and the ability to offer competitive supplemental benefits to a broader membership.
Plans achieving 4 Stars or higher retain access to quality bonus payments and can reinvest those dollars into richer benefits, impacting member acquisition, retention and stronger provider partnerships. Plans falling below the 4-Star threshold face a compounding disadvantage. Reduced rebate dollars limit benefit competitiveness. Over time, this creates a widening gap in both financial performance and market positioning.
The 2.48% rate increase outlined in the 2027 Medicare Advantage Rate Announcement does not expand the Stars bonus pool, and ongoing program changes are increasing downside risk for underperforming plans. As a result, Stars performance now directly determines not just quality outcomes, but a plan’s ability to compete and grow in an increasingly competitive Medicare Advantage market.
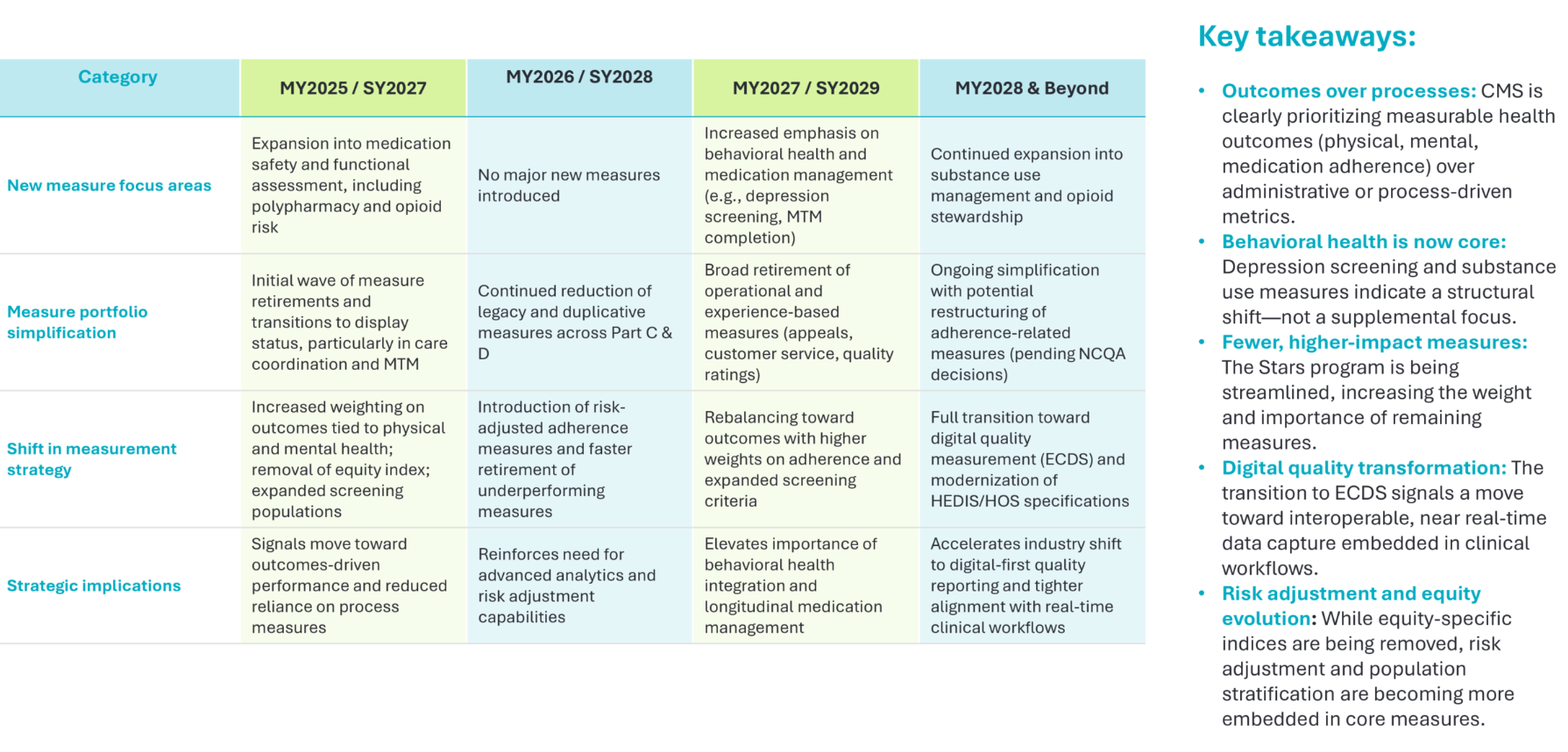
Summary of changes:
Strongly positioned for what’s ahead
The good news: plans and providers don’t have to navigate these changes alone. The 2027 Final Notice reinforces a shift the industry has been moving toward for years: execution at the point of care, grounded in clinical integrity and measurable outcomes. That’s where the capabilities of Cozeva + Vatica deliver.
Clinical validation, not administrative lift: Vatica’s service model places the PCP at the center of clinical coding, documentation and gap closure. This directly aligns with CMS’ move toward outcomes-based measurement and reduced reliance on administrative proxies. By ensuring that conditions are validated, documented and addressed during the encounter, providers can drive higher-integrity Stars performance while improving member care.
Unified risk and quality execution at the point of care: Cozeva’s technology platform operationalizes risk and quality workflows in a single, integrated experience, enabling clinical coding, documentation and gap closure during the patient encounter. As Stars increasingly rewards what happens during the visit itself, this approach ensures that every interaction is optimized for both clinical and financial performance.
Embedded behavioral health workflows: With behavioral health measures elevated in the 2027 model, structured workflows must support both visibility and action. Cozeva + Vatica technology surfaces behavioral health gaps in real time and enables providers to act through a workflow platform that can seamlessly integrate into the EHR.
EHR-native integration at scale: Both organizations integrate across major EHR platforms, embedding Stars execution directly into the provider workflow to minimize disruption and reduce administrative burden. This payer-agnostic approach allows providers to apply consistent workflows across a large portion of their Medicare Advantage population, driving adoption and scalability without adding operational complexity.
The direction from CMS is clear: success in Stars and risk adjustment will depend on the ability to deliver measurable health outcomes, supported by accurate, real-time documentation at the point of care. Plans that lead in 2027 and beyond will be those that equip their provider networks with the infrastructure to close gaps, capture behavioral health data and validate risk consistently and at scale.
If you’re looking for a partner that can activate providers where it matters most, the clinical encounter, Cozeva + Vatica is ready to help.